The COVID-19 crisis will exacerbate maternal and child undernutrition and child mortality in low- and middle-income countries

Published: July 2021
Publication: Nature Food
Authors: Saskia Osendarp, Jonathan Kweku Akuoku , Robert E. Black , Derek Headey, Marie Ruel , Nick Scott , Meera Shekar, Neff Walker, Augustin Flory , Lawrence Haddad, David Laborde , Angela Stegmuller , Milan Thomas and Rebecca Heidkamp
Read the original paper here.
Summary:
- COVID-related disruptions to food and health systems mean cases of malnutrition around the world are likely to get worse.
- People also have less money and therefor are turning to less expensive sources of calories such as starchy staples and eating fewer nutrient-dense foods.
- The study authors used statistical models to predict what these disruptions would do to malnutrition rates.
- They calculated “optimistic”, “moderate” and “pessimistic” outcomes.
- After the paper’s publication, the authors stated the pessimistic outcomes are the most likely.
- Using the pessimistic model as the authors recommend, they predict that by the end of 2022, COVID-19-related disruptions could result in an additional:
- 13.6 million wasted children
- 3.6 million stunted children
- 283,000 additional child deaths
- 4.8 million maternal anaemia cases
- 3 million children born to women with a low BMI
- US$44.3 billion in future productivity losses due to excess stunting and child mortality.
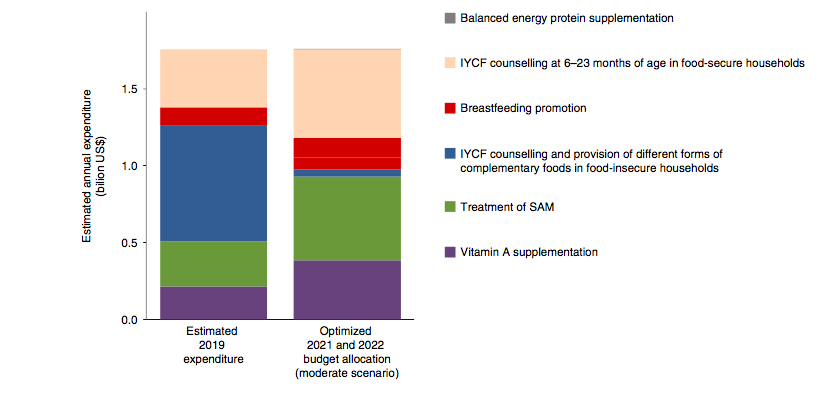
- To make up for the demands of the projected undernutrition increases, the authors predict we will need an additional $1.7 billion per year.
- The report also predicts that ODA for nutrition will be 19% less through 2030 than it would have been without COVID, accompanied by a similar decrease in domestic health budgets.
- We could save a lot of babies from being born small, preterm or stillbirth by a) switching the prenatal vitamins we give out from iron folic acid (IFA) to multiple micronutrient supplements (MMS) and b) Give balanced energy and protein supplements to malnourished pregnant women.
- The report argues1 that fewer children would be impacted if we move funding away from providing complementary foods and instead allocate resources toward:
- Balanced energy protein supplementation
- Breastfeeding promotion
- IYCF counseling at 6–23 months of age in food-secure households
- Wasting treatment
- Vitamin A supplementation
- These numbers should make it clear to decision makers that the pandemic is causing levels of undernutrition to rise in LMICs and that we need to urgently increase ODA and domestic funding to address this crisis.
Key Quotes:
- “The COVID-19 pandemic has created a nutritional crisis in LMICs. Without swift and strategic responses by subnational, national, regional and international actors, COVID-19 will not only reverse years of progress and exacerbate disparities in disease, malnutrition and mortality, but will also jeopardize human capital development and economic growth for the next generation.”
- “While women of reproductive age and young children are largely spared COVID-19’s direct effects (that is, serious disease and death), our projections demonstrate that, regardless of the scenario, the COVID-19 crisis is expected to have dramatic indirect effects on maternal and child undernutrition and child mortality in the current generation.”
- “The nutritional impacts of the COVID-19 crisis could have massive, long-term productivity consequences that could extend to future generations. Poor nutrition during early life stunts both physical and cognitive development, affects schooling performance and adult productivity, increases the risks of overweight/obesity and diet-related non-communicable diseases later in life, and triggers the intergenerational transmission of malnutrition.”
1 The article notes that “The optimal results and allocative efficiency gains will vary across countries, depending on demographics, epidemiological factors and baseline intervention coverages, as well as context-specific costs, priority targets, delivery platforms and other constraints.”








